IN A NUTSHELL
Author's note
 …My One Health analysis on Cambodia, Laos, Thailand, and Viet Nam has shown that there are gaps in the SDGs, primarily in the domesticated animal and crop realm that impact human health and well-being. Antimicrobial resistance, zoonotic diseases, food safety, food security (from the production standpoint), soil health, pesticide use, and animal waste management are important areas that are being overlooked. Livestock and their wastes produce methane and nitrous oxide, potent greenhouse gasses. Unexploded ordnances contaminating environments and killing innocent people are also not tracked. SDGs that specifically follow these areas would provide important information to improve global health, well-being, and sustainability…
…My One Health analysis on Cambodia, Laos, Thailand, and Viet Nam has shown that there are gaps in the SDGs, primarily in the domesticated animal and crop realm that impact human health and well-being. Antimicrobial resistance, zoonotic diseases, food safety, food security (from the production standpoint), soil health, pesticide use, and animal waste management are important areas that are being overlooked. Livestock and their wastes produce methane and nitrous oxide, potent greenhouse gasses. Unexploded ordnances contaminating environments and killing innocent people are also not tracked. SDGs that specifically follow these areas would provide important information to improve global health, well-being, and sustainability…

By Laura H. Kahn, MD, MPH, MPP
Co-Founder, One Health Initiative
Examining the U.N. Sustainable Development Goals (SDGs) Using a One Health Approach: Profiling Cambodia, Laos, Thailand, and Viet Nam
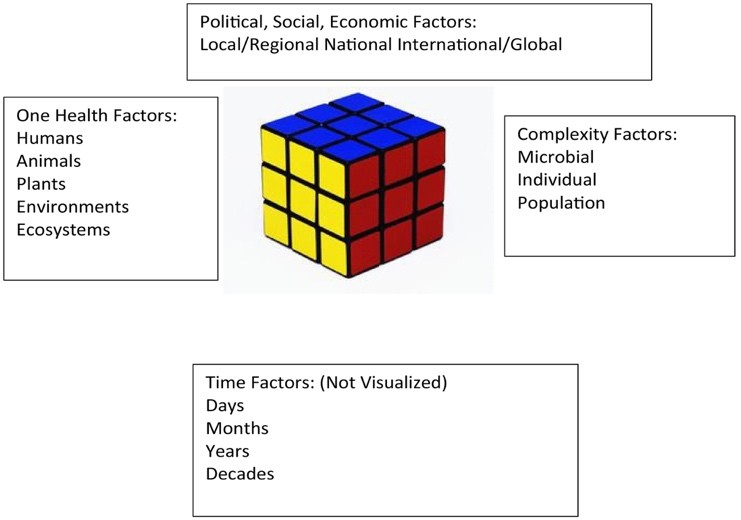
In 2024, I compared the Ecuadorian Amazon Rainforest to the Galapagos Islands using a One Health approach. One Health is the concept that human, animal, plant, environmental and ecosystem health are linked. This concept can be visualized as a multi-dimensional matrix, assisting health professionals, researchers, and policy makers to analyze and address complex health challenges in a concise, systematic, and comprehensive way.
One Health Multi-dimensional Matrix:
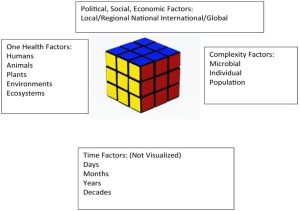
In this paper, I will use the One Health matrix as a lens to evaluate five of the United Nation’s Sustainable Development Goals (SDGs) as they pertain to four Southeast Asian countries: Thailand, Laos, Cambodia, and Vietnam. The five SDGs are: 2. Zero Hunger, 3. Good Health and Well Being, 6. Clean Water and Sanitation, 15. Life on Land, and 16. Peace, Justice, and Strong Institutions. Each of these SDGs has targets and indicators. An example of a target is SDG 6.1: By 2030, achieve universal and equitable access to safe and affordable drinking water for all. The indicator for this target is: Proportion of population using safely managed drinking water services. Targets typically have two or more indicators which are tracked over time. The trends are either positive, negative, or neutral.
United Nations Sustainable Development Goals:
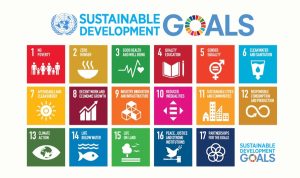
The SDGs were developed in 2012, at a United Nations Conference on Sustainable Development in Rio de Janeiro, Brazil. The delegates created seventeen SDGs to reduce hunger, disease, deforestation, biodiversity loss, and other global issues by 2030. Since 2016, the UN’s Department of Economic and Social Affairs has issued annual SDG Reports, which evaluate progress towards the goals using indicator trends. For example, Goal 2: Zero Hunger has targets for success including ending malnutrition, stunting, and wasting in children under age 5. Goal 3. Good Health and Well-Being has targets that seek to reduce rates of mortality in infants, new mothers, children, and other groups as well as reducing rates of infectious and chronic diseases. For Goal 15. Life on Land, the targets range from halting deforestation to ending poaching and trafficking of endangered species. Other SDGs also involve One Health elements (i.e., SDGs 11, 12, 13, and 14), but for the sake of time, will not be included in this analysis.
The 2024 report, released on June 28th, found that while some of the SDGs have made progress, such as preventing HIV infections and improving education access for girls, others have fallen short or have regressed, particularly in the wake of the Covid-19 pandemic. Problematic areas include worsening food insecurities, diminishing vaccine delivery to children, worsening access to clean water and sanitation, escalating geopolitical conflicts, and increasing species extinction risks. Country Profiles of the 17 SDGs targets and indicators for the 193 UN Member States highlight the trends.
Since I recently visited the Southeast Asian countries of Cambodia, Laos, Thailand, and Vietnam, I will examine them at the population level using the One Health matrix and compare the findings with the SDGs.
To understand the political, social, and economic factors of Cambodia, Laos, Thailand, and Vietnam, we must first briefly review the history of the region.
Brief Historical Background
The ancient Khmer empire (802 CE to 1431 CE) of Cambodia encompassed much of the region that would subsequently become Thailand and Laos, influencing their languages, cultures, and traditions. In the mid-14th century, a Tai army attacked the Khmer empire’s capital at Angkor, contributing to its decline, and eventually becoming a Tai vassal state. The Khmer empire was succeeded by the Ayutthaya Kingdom (1351 to 1767) which became the precursor of modern Thailand.
Of the four countries, only Thailand avoided being colonized by European powers. Britain and France decided that Thailand would provide a useful buffer zone between the British colony of Burma and the French colony of Indochina. During World War 2, Thailand was under the rule of a military dictator named Phibunsongkhram, aka Phibun, who allowed Imperial Japan to build its infamous Thailand-Burma Railway, nicknamed the “death” railway within its borders. After the war, resistance groups forced Phibun to resign. Thailand subsequently became a pro-Western country, allying with the U.S. during the Cold War, and benefitting financially from U.S. economic and military aid during the Vietnam War.
In contrast to Thailand, Vietnam had been colonized by a succession of Chinese dynasties for 1000 years, from 111 BC to 939 AD, enduring a long history of warfare. From the 11th to 18th centuries, Vietnam conquered parts of the Khmer empire and spread southward, but outbreaks of fighting between different war lords developed. France established a colony in Vietnam after assisting one of the war lords, and by the late 19th century, it had gained control of Vietnam, Cambodia, and Laos, calling the region French Indochina. France used the colonies for their natural resources.
Resistance movements began soon after the French takeover.
Ho Chi Minh (1890-1969) was the leader of a major Vietnamese resistance movement, advocating for the independence of Indochina, and became a founding member of the Vietnamese Communist Party. He sought assistance from delegates at the Versailles peace conference at the end of World War I but was rebuffed.
At the end of World War II, he sought help from President Harry S. Truman for independence from French rule. Truman sided with the French. With Chinese assistance, Vietnamese Communist troops, called the Viet Minh, defeated the French at the Battle of Dien Bien Phu in 1954. Indochina was divided into communist North Vietnam, non-communist South Vietnam, Cambodia, and Laos. One year later, Ho Chi Minh visited Moscow and secured economic and military aid from Leonid Brezhnev. This sequence of events led to war in Southeast Asia (1961-1973) as the U.S. sought to contain the spread of communism. The North Vietnamese and their allies defeated the U.S. which was forced to withdraw.
The U.S. heavily bombed Cambodia and Laos during the war in Vietnam. Civil war broke out in Cambodia, and in 1975, Pol Pot, the Communist leader of the Khmer Rouge seized control and began persecuting those whom the communists considered tainted by capitalism. Over the next four years, the Khmer Rouge committed genocide, killing over 1.7 million people. The Vietnamese invaded in 1979 and removed the Khmer Rouge from power. The horrors of the Khmer Rouge regime have inflicted long lasting traumas on the Cambodian people. Laos endured a secret war lasting from 1964 to 1973 during which time the U.S. bombed large areas of the country. The unexploded ordnances (UXO) contaminate the land and continue to kill innocent people.
Political, Social, and Economic Factors and SDG 16.
Of the four countries, only Thailand escaped war with the U.S. and its bombing campaigns. Both Vietnam and Cambodia experienced civil war, but Cambodia alone endured the 5-year genocide involving 47% of its people. The survivors and their descendants continue to bear the scars of the atrocities. Cambodia has the lowest Human Development Index score even though Laos has the lowest GDP per capita. The Human Development Index is a composite score for life expectancy, education level attainment for adults aged 25 years, and gross national income per capita. None of the SDGs use the HDI as an indicator.
Vietnam, a communist country, has the highest Happiness Index score. Their social cohesion appears high. The Happiness Index is based on a survey of subjective well-being by the Gallup World Poll. None of the SDGs use the Happiness Index as an indicator.
Transparency International is a nongovernmental organization with the mission to stop corruption and promote transparent and responsible government. Of the four countries, the Vietnamese consider their country the least corrupt, with a Corruption Perception Index (CPI) score of 41/100, compared to the other three countries which have lower scores. Cambodians ranked their country as the most corrupt (CPI score 22). Thailand is the wealthiest of the four countries economically. It is considered moderately corrupt with a CPI score of 35/100 but ranked moderately happy. SDG 16. Peace and Justice targets 16.5 – 16.8 track corruption using the CPI.
(In comparison, Denmark and Finland are the least corrupt countries in the world, scoring 90 and 87, respectively, and they are the world’s happiest countries.)
The One Health matrix’s third dimension of political, social, and economic factors overlaps with SDG 16 which has targets such as: reducing rates of corruption, improving transparent government, and enforcing laws and policies for sustainable development.
Please see Table 1 below
One Health Factors and SDGs 2, 3, 6, 15
Vietnam has the largest population and highest population density in the Greater Mekong Delta region. (Note: The region is named after the Mekong River which flows through all four countries as well as China, and Myanmar.)
SDG 2. Zero Hunger targets include prevalence rates of undernourishment or food insecurity, volume of food production, and agriculture orientation index of government expenditures, and agricultural export subsidies, among others. It does not include UN Food and Agriculture Organization data such as crop yields or national livestock inventories. The focus is on food consumption but not on food production.
Thailand has the most land surface area followed by Vietnam, Laos, and Cambodia. It also has the most arable land for agriculture. Vietnam has less than half the arable land area as Thailand, but it is an agricultural powerhouse, being one of the largest producers of rice and coffee in the world.
Although food safety is briefly mentioned in Target 2.1, none of the indicators specifically track foodborne illness rates.
Food waste is tracked in SDG 12 by a food loss index and the food waste index.
SDG 3. Good Health and Well-Being. Thailand and Vietnam have comparable life expectancies although Thailand spends over two times more on healthcare per capita than Vietnam. Both countries have lower crude death rates, infant mortality rates, and fertility rates than Cambodia and Laos. Laos has the highest infant mortality rate and lowest life expectancy of the four countries. It spends five times less on healthcare per capita than Thailand. SDG 3. follows these metrics, but its targets do not include One Health issues such as reducing antimicrobial resistance or zoonotic diseases such as rabies, particularly in dogs, which is a major problem in the region.
In 2023, the WHO listed antimicrobial resistance as one of the top global public health and development threats in the world, directly responsible for an estimated 1.27 million deaths and indirectly responsible for almost 5 million deaths in 2019. Misuse and overuse of antimicrobials occur in human, animal, and plant health. It is a major One Health issue that includes environmental and ecosystem health. In 2015, WHO launched the Global Antimicrobial Resistance and Use Surveillance System (GLASS) to track global antimicrobial consumption using a One Health surveillance model. As of 2022, WHO provides profiles of the member countries.
Dengue is a deadly mosquito-borne disease. Over 7.6 million cases were reported to WHO in 2024. Rates have been increasing, and with climate change, are likely to get worse. WHO began a global surveillance database for dengue.
The SDGs track malaria, tuberculosis, HIV, and neglected nontropical diseases, but they do not track rabies, a deadly zoonotic disease that causes almost 60,000 deaths in over 150 countries, particularly in Africa and Asia. Rabies is a major problem in Southeast Asia. The virus is usually spread by dog bites.
SDG 6. Clean Water and Sanitation. The targets include the proportion of a population that has access to safe drinking water and sanitation facilities that dispose of human waste. Sanitation systems are designed to process human waste, not animal waste. Animal waste, particularly domestic animal waste, is typically not processed even though most fecal waste produced is from animals. Animal waste contaminates waterways and crops and contributes to water and foodborne illnesses. It might also be a source of antimicrobial resistant pathogens, particularly in Southeast Asia.
SDG 15. Life on Land. Laos is the only country that is landlocked, but it has the highest percentage of forested land. Cambodia has the highest deforestation rate followed by Vietnam, Laos, and Thailand.
All four countries have moderately poor air quality, but Thailand and Vietnam have the best water quality. Measurements of soil quality have yet to be published.
Endangered species are listed by taxonomic groups in the “Red List Index.” These groups include amphibians, mammals, cycads, and warm-water reef-forming corals. Endangered sentinel species are not profiled. The World Wildlife Fund considers elephants and tigers to be endangered sentinel species in the Greater Mekong region. Laos was once known as the “Land of a Million Elephants” because historically it had the most wild elephants. In the latest count, the country had approximately 400 wild elephants left. Vietnam had less than 200 while Thailand had over 3,000. Wild tigers are extinct in Cambodia, Laos, and Vietnam. Less than 250 tigers exist in Thailand. People care about specific charismatic animals, such as elephants and large cats. Tracking an endangered species index is vitally important, but profiling specific endangered animals that people feel passionate about might be equally important.
Please see Table 2 below
One Health Matrix Identified SDG Gaps
No Human Development Index (HDI) -life expectancy, income, education.
No Happiness Index—a measure of social well-being.
Food Security is tracked by consumption and less so on production.
No Food Safety or Foodborne Illness rates are tracked. (SDG 12 includes Food Loss and Food Waste)
Specific Antimicrobial Resistance (AMR) rates in humans or animals are not tracked.
Zoonotic diseases such as rabies death rates are not tracked.
Vaccination Rates in animals, such as canine vaccination rates against rabies, are not tracked.
Domestic Animal Health (e.g., cats, dogs, or livestock) is not represented in SDGs.
Soil health is not tracked.
Crop production and yields are not tracked.
Livestock production and yields are not tracked.
Pesticide use in crops is not tracked.
There is no Domestic Animal Waste Production Index
There is no Domestic Animal Waste Management Index.
Specific Endangered Sentinel Wildlife are not tracked.
Unexploded ordnances not tracked in war-torn nations.
Conclusions
Colonization and war have severe consequences for a nation’s health, wealth, and well-being. The history of the four Southeast Asian countries profiled in this paper illustrates this point. Thailand was never colonized and avoided war. From a One Health perspective, its people, animals, and environments are faring the best, although Vietnam, despite its war-torn history, is a close second. The fact that Vietnam defeated the United States during the 20th century war is a likely explanation for the optimism, social cohesion, and dynamism of its people. Comparing the Corruption Perceptions Index and Happiness Index of the four countries finds that Vietnam ranks the highest of these two measures even though Thailand is technically the wealthiest of the four based on its GDP and Health Expenditures.
My One Health analysis has shown that there are gaps in the SDGs, primarily in the domesticated animal and crop realm that impact human health and well-being. Antimicrobial resistance, zoonotic diseases, food safety, food security (from the production standpoint), soil health, pesticide use, and animal waste management are important areas that are being overlooked. Livestock and their wastes produce methane and nitrous oxide, potent greenhouse gasses. Unexploded ordnances contaminating environments and killing innocent people are also not tracked. SDGs that specifically follow these areas would provide important information to improve global health, well-being, and sustainability.
The 17 UN SDGs represent a global vision to improve life on Earth for all countries and for all peoples. Tracking the many targets and indicators over the years has been a monumental effort and a testament to the commitment by the international community to achieve these goals. The challenges of the 21st century will make these efforts increasingly important. A One Health approach should be included to ensure healthy animals, plants, environments, and ecosystems.
Table 1. Political, Social, Economic Factors
Table 2. One Health Factors at Population Levels
| Country |
Cambodia |
Laos |
Thailand |
Vietnam |
| Humans |
|
|
|
|
| Population |
17.6 million |
7.8 million |
71.7 million |
100.9 million |
| Population Density (people per km2) |
100 |
34 |
140.1 |
328 |
| Estimate of total human fecal production (kg/yr) |
1.9 X 109 |
8.5 X 108 |
7.8 X 109 |
8.9 X 109 |
| Life Expectancy for Both Sexes in Years (2024) |
70.82 |
69.23 |
76.56 |
74.74 |
| Total Fertility Rate (Live Births per Woman) (2024) |
2.5 |
2.4 |
1.2 |
1.9 |
| Infant Mortality Rate, Both Sexes, Probability of Dying Between Birth and Age 1 per 1000 Live Births (2022) |
20.3
|
32.7
|
7.0 |
16.2 |
| Crude Death Rate per 1,000 population |
6.78 |
6.05 |
5.05 |
5.5 |
| Dengue (total reported cases, 2024) |
18,983 |
19,486 |
104,681 |
103,078 |
| Rabies, reported human deaths 2022 |
No data, but reportedly has one of the highest death rates in the world from rabid dog bites. |
20 |
3 |
70 |
| Animals (Domestic Livestock and Sentinel Wildlife Species) |
|
|
|
|
| Dogs (2021/2023) |
5 million |
Est. 5 million |
12.8 million |
5.5 million |
| Chickens (per 1000 animals) (2023) |
12,817 |
52,235 |
288,758 |
457,221 |
| Ducks (per 1000 animals) (2023) |
8,878 |
3,693 |
15,504 |
87,645 |
| Buffalo (2023) |
665,269 |
1,211,949 |
889,775 |
2,136,009 |
| Cattle (2023) |
2,611,835 |
2,542,707 |
4,630,798 |
6,331,895 |
| Goats (2023) |
Est.400,000 |
786,965 |
483,417 |
3,088,328 |
| Horses (2023) |
31,585 |
32,000 |
7,230 |
48,821 |
| Pigs/Swine (2023) |
2,036,958 |
4,525,574 |
7,721,375 |
25,546,030 |
| Estimated Total Domestic Animal Fecal Waste (kg/year) |
2.6X109 |
3.7X109 |
7.0X109 |
13.6X109 |
| Wild Elephant Population |
400 to 600 |
400 |
3,084-3,500 |
<200 |
| Wild Tiger Population |
Extinct |
Extinct |
179-223 |
Extinct |
| Plants (Domestic) |
|
|
|
|
| Arable Land for Agriculture
(hectares) 2022 |
4,120 |
1,224 |
17,150 |
6,754 |
| Coffee, green (2023) |
365 tons |
177,662 tons |
16,575 tons |
1,956,782 tons |
| Rice (2023) |
12,900,000 tons |
3,835,000 tons |
33,070,957 tons |
43,497,625 tons |
| Environments and Ecosystems |
|
|
|
|
| Air Quality.
Average Particulate Matter 2.5 microns (PM2.5),
2023 |
73 ug/m3 (Moderate)
|
88 ug/m3 (Moderate)
|
74 ug/m3
(Moderate)
|
88 ug/m3 (Moderate)
|
| Water Quality. Environmental Performance Index (EPI) 2023 |
40.0 |
32.2 |
51.3 |
54.3 |
| Soil Quality |
Asian Soil Laboratory Network (SEALNET), established in 2017, has not yet issued a report. |
| Percent Land Contamination with unexploded ordnance (UXO) |
>20% |
>20% |
Along Thai-Cambodian border |
>20% |
|
|
|
|
|
|
|
|
|
Methodology used to calculate human and animal fecal waste production based on 2018 Nature Sustainability paper by Berendes, et al. ChatGPT used to estimate adult human and animal body weights and to calculate fecal production per human and animal populations.
__
By the same Author on PEAH
Lessons From Ecuador: A One Health Perspective
















{kind=link}