IN A NUTSHELL
Authors's note
 This article discusses about the Stop Cannabis Challenge app developed by The Centre for Addiction and Mental Health (CAMH) to support tolerance breaks and cannabis abstinence. This app promotes cannabis addiction awareness and provides cessation support through health education and intervention
This article discusses about the Stop Cannabis Challenge app developed by The Centre for Addiction and Mental Health (CAMH) to support tolerance breaks and cannabis abstinence. This app promotes cannabis addiction awareness and provides cessation support through health education and intervention

Splash screen of the Stop Cannabis Challenge App
By
Nejat Hassen(1), Dr. Mohita Chadha(2), Dr. Michael Chaiton(3), Dr. Sumedha Kushwaha(4)
1-Student, Healthcare Management Program, Longo Faculty of Business, Humber College
2-Chief Operating Officer, Global Initiative for Public Health and Innovation
3-Independent Scientist, Center for Addiction and Mental Health
4-Research Assistant, Center for Addiction and Mental Health
Toronto, Ontario, Canada
ARE YOU NOT ADDICTED TO CANNABIS? PROVE IT
Canada is facing a serious mental health crisis alongside rising substance abuse and dangerous drug use. Substance abuse is influenced by many complex factors often beyond individual control (P. H. A. of Canada, 2021). The Cannabis Act, effective October 17, 2018, regulates access, production, distribution, and sale of cannabis. The 2023 Canadian Cannabis Survey reported an increase in cannabis use from 22% in 2018 to 26% in 2023 (H. Canada, 2021).
Cannabis contains two main components: THC and CBD (Zehra et al., 2018). While not everyone who uses cannabis becomes addicted, frequent and long-term use, especially starting in early adolescence, can lead to addiction. Cannabis Use Disorder (CUD) is defined as the inability to stop using cannabis despite it causing harm. About 10% of the 193 million global cannabis users are affected by CUD (Connor et al., 2021).
In 2016, about 22.1 million people worldwide met the criteria for CUD (The Global Burden of Disease Attributable to Alcohol and Drug Use, 2018). Problematic cannabis use includes behaviors like neglecting major duties, giving up important activities, using more cannabis than intended, and being unable to cut down on use. Withdrawal symptoms, both mental and physical, can occur when frequent users stop, increasing the risk of relapse (H. Canada, 2018b).
Treating CUD is complicated by other mental health and substance use disorders. Cognitive behavioral therapy, motivational enhancement therapy, and contingency management can reduce cannabis use, but long-term abstinence is rare (Connor et al., 2021). Legalizing non-medical cannabis could increase CUD by making potent cannabis more accessible and cheaper. Education on the risks and help-seeking is crucial.
Engaging young people with CUD is challenging, but digital interventions show promise. Technology can effectively reach many people, helping to prevent, screen, and treat CUD (Brezing & Levin, 2022). Mobile technology offers new ways to address substance use disorders, including cannabis cessation.
We developed the “Stop Cannabis Challenge” app with The Centre for Addiction and Mental Health (CAMH) to support tolerance breaks and cannabis abstinence. This app promotes cannabis addiction awareness and provides cessation support through health education and intervention.
App Description
- Abstinence Tracker: allows users to track the time since they last used cannabis. The time is displayed in days, hours and minutes. This serves as a motivational tool by visually representing their progress and encouraging longer periods of abstinence.
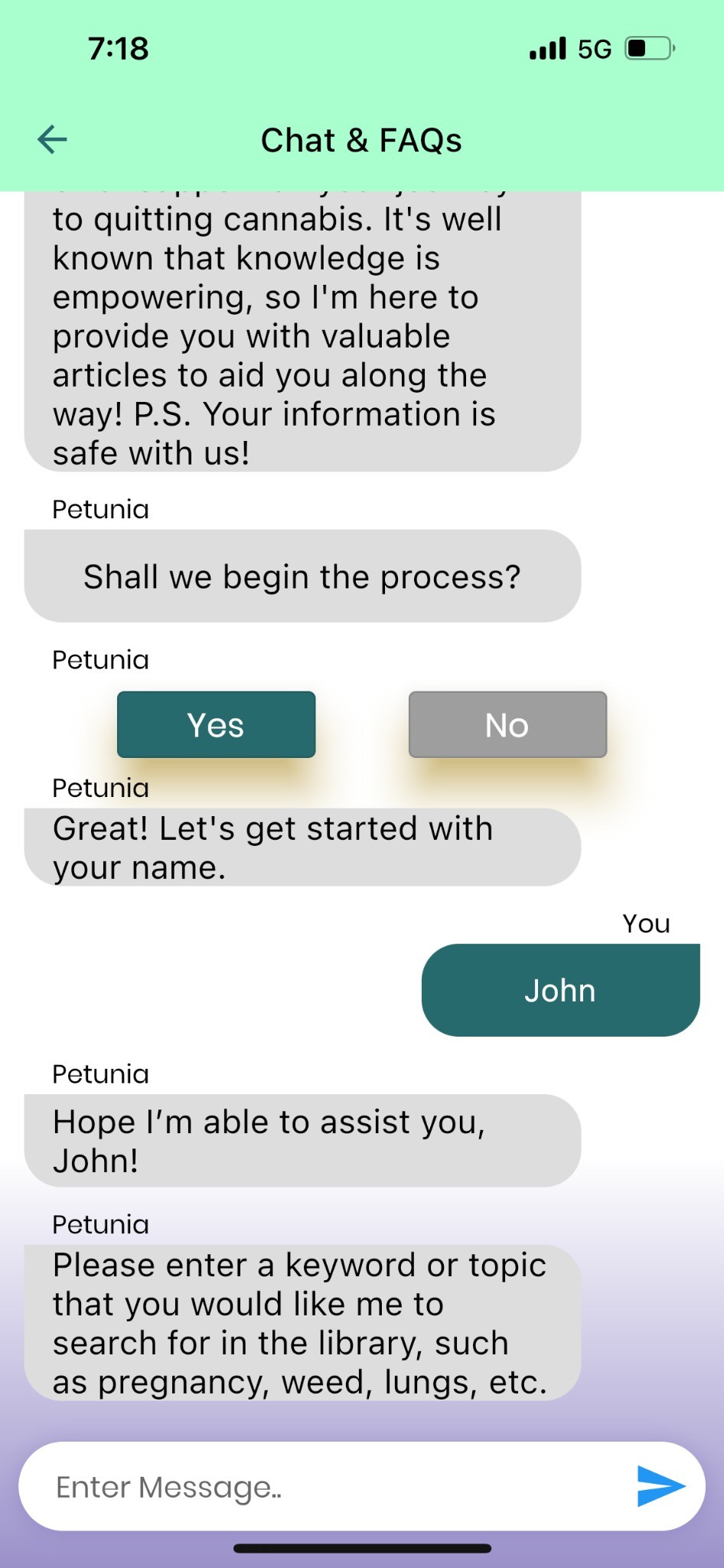
- Chatbot Enabled FAQ Section: a 24/7 chatbot offers users instant access to information on various topics related to cannabis use and cessation. This ensures users receive timely support and answers to their questions at any hour.
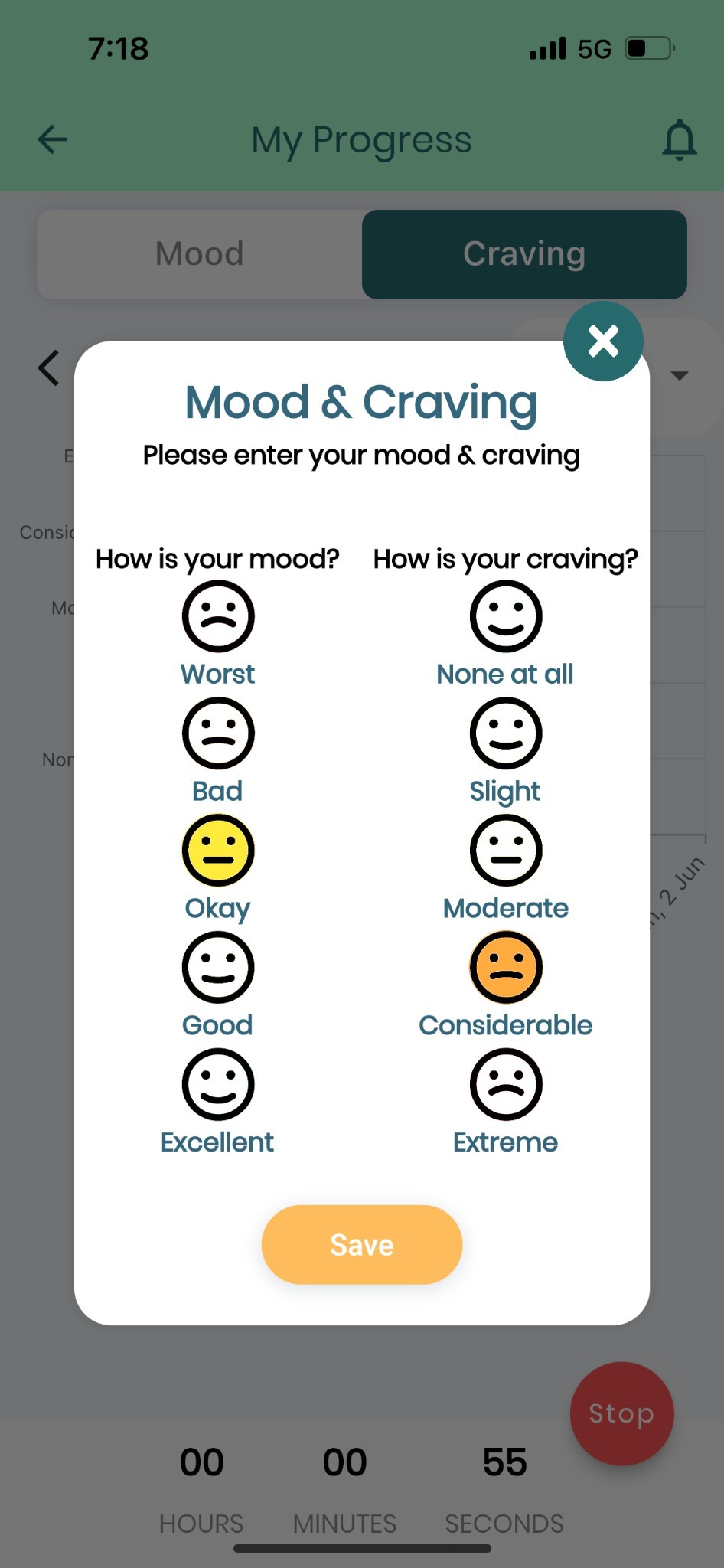
- Mood and Craving Tracker: records daily moods and cravings with graphical representations of their emotional and physical states. Analyzing this data on a weekly and monthly basis helps users identify patterns and triggers that may affect their cessation journey.
- Invite Friends: The app enables users to send invitations to both registered and non-registered users, fostering a supportive community. Users can view friend requests received and send out invitations, building a network of support crucial for successful cessation.
- Leaderboard: To offer positive reinforcement, the app includes a leaderboard that ranks users and their friends based on a complex algorithm. It motivates users to remain committed to their goals by seeing their progress with others.
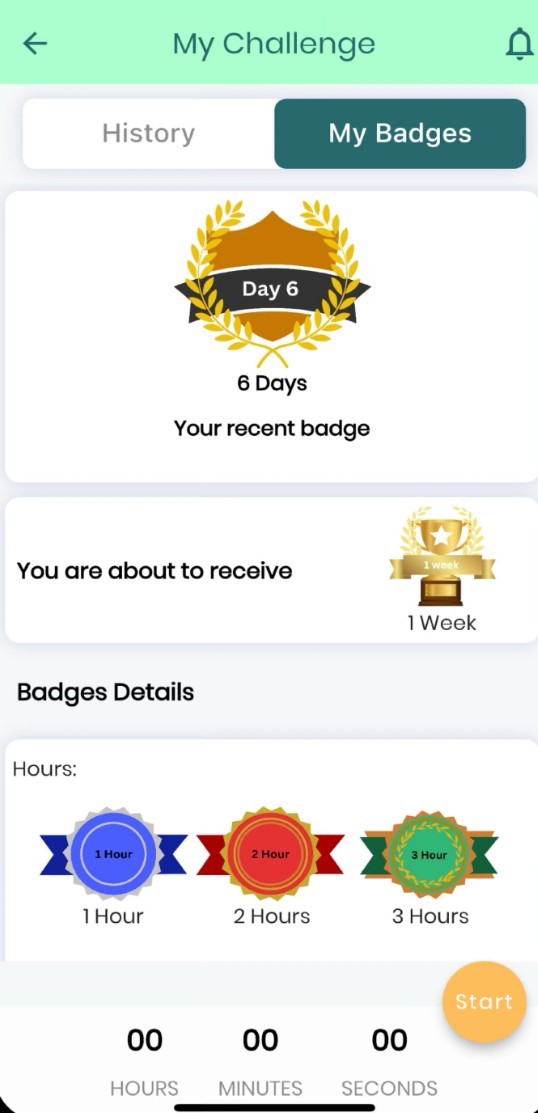
- Challenge History and Badges: Users earn badges as they progress, categorized by hours, days, and weeks of abstinence. This provides reward milestones and summaries of current and previous challenges.
- Motivational Messages: Automated daily motivational messages are sent as in-app notifications to inspire users, offering encouragement and positive reinforcement throughout their cessation journey.
- Baseline Stop Cannabis Survey: The Cannabis Use Disorder Identification Test-Revised (CUDIT-R) has a set of 16 questions which are present to the newly registered user to assess cannabis dependence and its problematic use.
- Ecological Momentary Assessment (EMA): is presented each time the user stops the abstinence tracker. It aims to collect multiple responses around cannabis withdrawal, peer cannabis use, reasons for use, craving, location during cannabis use, and feedback of the user.
Can technology be used?
Research shows digital interventions can effectively reduce substance use. Several studies have found significant reductions in substance use behaviours through digital tools. For instance, a systematic review of digital interventions aimed at reducing substance misuse among students found significant reductions in substance use behaviours, emphasizing the positive impact on health, social, and economic problems (Dick et al., 2019). A specific randomized controlled trial focusing on an Internet-based intervention to reduce cannabis use (ICan) showed that participants in the intervention group experienced significant reductions in cannabis use compared to the control group, highlighting the potential of digital tools to aid in substance use reduction (Olthof et al., 2021).
Qualitative feedback from users of digital interventions often underscores their acceptability and usefulness. Users find these tools easy to use and appreciate the anonymity and accessibility they provide. Participants have reported positive experiences, including improved self-efficacy and overall quality of life (Jormand et al., 2022).
Conclusion
The Stop Cannabis Challenge app represents a valuable tool in the fight against cannabis addiction. By evaluating its feasibility and efficacy through studies and user feedback, we can improve the app and enhance public health outcomes in Canada. Engaging users through co-creation and integrated knowledge translation ensures the app meets their needs and maximizes its effectiveness. This app is a significant step forward in digital health interventions for cannabis cessation, offering a reliable, user-friendly tool to support individuals in their efforts to quit cannabis. A feasibility study will help refine the app and contribute to the broader field of substance use disorder treatment, ultimately improving public health.
References
Brezing, C. A., & Levin, F. R. (2022). Applications of technology in the assessment and treatment of cannabis use disorder. Frontiers in Psychiatry, 13, 1035345. https://doi.org/10.3389/fpsyt.2022.1035345
Canada, H. (2018a, March 2). Addiction to cannabis [Education and awareness]. https://www.canada.ca/en/health-canada/services/drugs-medication/cannabis/health-effects/addiction. html
Canada, H. (2018b, October 17). Is cannabis addictive? [Research;education and awareness]. https://www.canada.ca/en/health-canada/services/publications/drugs-health-products/cannabis-addicti ve.html
Canada, H. (2021, December 16). Key findings: Cannabis use in Canada (2023) — Canada.ca [Datasets;statistics;education and awareness;interactive resource;]. https://health-infobase.canada.ca/cannabis/
Canada, P. H. A. of. (2021, December 15). Statement from the Minister of Mental Health and Addictions on the Overdose Crisis [Statements]. https://www.canada.ca/en/public-health/news/2021/12/statement-from-the-minister-of-mental-health-and-addictions-on-the-overdose-crisis.html
Connor, J. P., Stjepanović, D., Le Foll, B., Hoch, E., Budney, A. J., & Hall, W. D. (2021). Cannabis use and cannabis use Disorder. Nature Reviews. Disease Primers, 7(1), 16. https://doi.org/10.1038/s41572-021-00247-4
Dick, S., Whelan, E., Davoren, M. P., Dockray, S., Heavin, C., Linehan, C., & Byrne, M. (2019). A systematic review of the effectiveness of digital interventions for illicit substance misuse harm reduction in third-level students – BMC public health. BioMed Central. https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-019-7583-6
Elsbernd, A., Hjerming, M., Visler, C., Hjalgrim, L. L., Niemann, C. U., Boisen, K. A., Jakobsen, J., & Pappot, (2018). Using Cocreation in the Process of Designing a Smartphone App for Adolescents and Young Adults With Cancer: Prototype Development Study. JMIR Formative Research, 2(2), e23. https://doi.org/10.2196/formative.9842
Government of Canada, C. I. of H. R. (2012, December 6). Guide to Knowledge Translation Planning at CIHR: Integrated and End-of-Grant Approaches – CIHR. https://cihr-irsc.gc.ca/e/45321.html
ICD-11 for Mortality and Morbidity Statistics. (n.d.). Retrieved February 28, 2024, from https://icd.who.int/browse/2024-01/mms/en
Jormand, H., Bashirian, S., Barati, M., Rezapur-Shahkolai, F., & Babamiri, M. (2022). Evaluation of a web-based randomized controlled trial educational intervention based on media literacy on preventing substance abuse among college students, applying the Integrated Social Marketing Approach: A study protocol – trials. BioMed Central. https://trialsjournal.biomedcentral.com/articles/10.1186/s13063-022-06913-6
Olthof, M. I. A., Blankers, M., Laar, M. W. van, & Goudriaan, A. E. (2021). ICAN, an internet-based intervention to reduce cannabis use: Study protocol for a randomized controlled trial – trials. BioMed Central. https://trialsjournal.biomedcentral.com/articles/10.1186/s13063-020-04962-3
Kroon, E., Kuhns, L., Hoch, E., & Cousijn, J. (2020). Heavy cannabis use, dependence and the brain: A clinical perspective. Addiction (Abingdon, England), 115(3), 559–572. https://doi.org/10.1111/add.14776
The global burden of disease attributable to alcohol and drug use in 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. (2018). The Lancet. Psychiatry, 5(12), 987–1012. https://doi.org/10.1016/S2215-0366(18)30337-7
Zehra, A., Burns, J., Liu, C. K., Manza, P., Wiers, C. E., Volkow, N. D., & Wang, G.-J. (2018). Cannabis Addiction and the Brain: A Review. Journal of Neuroimmune Pharmacology, 13(4), 438–452. https://doi.org/10.1007/s11481-018-9782-9
SCREENSHOTS

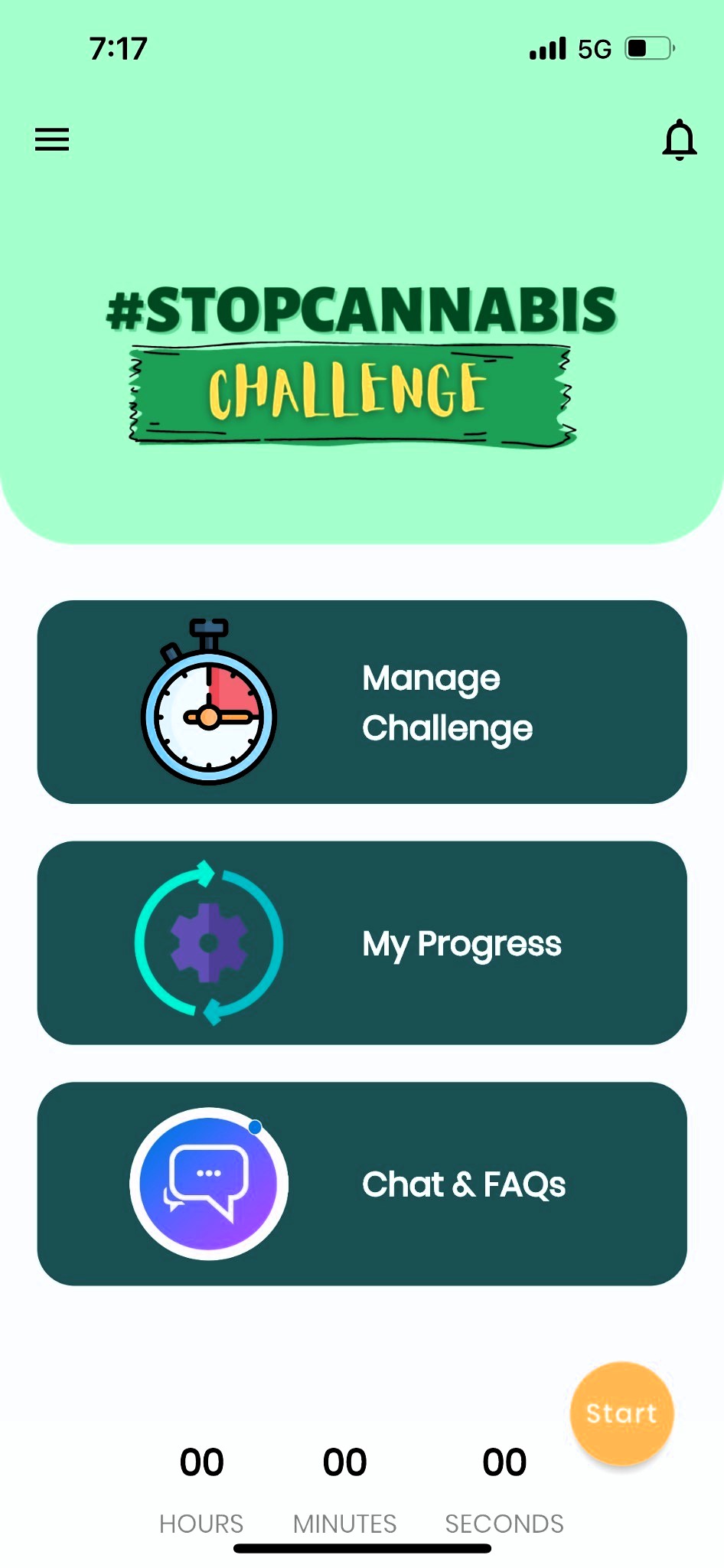
Homepage displaying Manage Challenge which allows users to track the time since they last used cannabis, My Progress which records daily moods and cravings with graphical representations of their emotional and physical states, Chat & FAQs, a 24/7 chatbot offers users information on various topics related to cannabis use and cessation

Chatbot Enabled FAQ Section: a 24/7 chatbot offers users instant access to information on various topics related to cannabis use and cessation. This ensures users receive timely support and answers to their questions at any hour

Mood and Craving Tracker records daily moods and cravings with graphical representations of their emotional and physical states. Analyzing this data on a weekly and monthly basis helps users identify patterns and triggers that may affect their cessation journey

Abstinence Tracker: allows users to track the time since they last used cannabis. The time is displayed in days, hours and minutes. This serves as a motivational tool by visually representing their progress and encouraging longer periods of abstinence
Challenge History and Badges: Users earn badges as they progress, categorized by hours, days, and weeks of abstinence. This provides reward milestones and summaries of current and previous challenges