Authoritative insights by 2017 PEAH contributors added steam to debate on how to settle the conflicting issues that still impair equitable access to health by discriminated population settings worldwide

by Daniele Dionisio*
PEAH – Policies for Equitable Access to Health
2017: a Year in Review through PEAH Contributors’ Takes
Now that 2017 just came to its end, I wish to thank the top thinkers and academics who enthusiastically contributed articles over the year. Their authoritative insights meant a lot to PEAH scope while adding steam to debate on how to settle the conflicting issues that still impair equitable access to health by discriminated population settings worldwide.
Find out below a list of links and relevant summaries:
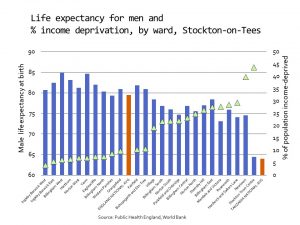
By Ted Schrecker Professor of Global Health Policy, Durham University, UK
...health researchers and professionals are (or should be) asking how Brexit will, and could, affect public health. Among the questions, informed by a political economy perspective on health and its social determinants, five stand out.One needs to remind oneself that the last word in Albert Camus’ famous essay about suicide is ‘hope’. But it is hard to sustain in these times
By Claudio Schuftan People’s Health Movement – PHM
Donor countries (the US in particular) continue to push WHO towards working with industry through ‘multi‐stakeholder partnerships’, rather than giving WHO the chance to implement regulatory and fiscal strategies that could make a real difference. Moreover, bilateral donors (and big philanthropies) demand WHO provides data according to their particular interests. Therefore, the types of data produced by WHO (and other UN agencies) are greatly influenced by a donor mandate that goes beyond the simple compilation of country-reported statistics
By Olesya Kravchuk Communications Officer at AFEW (AIDS Foundation East-West) International
Tajikistan is among the countries where HIV prevalence has increased by more than 25% over the last 10 years. In Tajikistan the number of sterile needles and other commodities for people who inject drugs per year is still very low. AFEW-Tajikistan is the only NGO in the country that has HIV voluntary counselling and rapid testing
By Renée de Jong Junior Global Health Advocate at Wemos Foundation
The WHO model for Health System Strengthening (HSS) includes improving its six health system building blocks and managing their interactions in ways that achieve more equitable and sustained improvements across health services and health outcomes.... It appears that Gavi maintains a very different interpretation of HSS....vhere the interconnectedness between the building blocks is hardly taken into account
By Alex Henriquez Research Analyst at Healthcare Improvement Scotland / Scottish Health Council
A really equitable health system is that that ensures that people with special needs also have fair access to healthcare. This is especially relevant for people with communication needs, who may experience more barriers of access to healthcare services. Inclusive communication is an approach to communication in which information and its understanding are made accessible to everyone
By Lauranne Botti, Manager, and Carel Ijsselmuiden, Executive Director, COHRED’s Research Fairness Initiative (RFI)
The Research Fairness Initiative (RFI) responds to the increasing understanding of the importance of partnerships and SDG 17 by ensuring that institutions around the world can have access to an evidence-base on how to create and maintain fair, trustworthy and equitable partnerships in research and innovation
By Lawrence C. Loh Dalla Lana School of Public Health, University of Toronto, and Director of Programs at The 53rd Week Ltd
The observed increase in violence against physicians is a clear trend, supplemented by no end of anecdotal stories of physician disrespect; spitting, verbal, and physical assault, online harassment. Many of these would be criminal if done against a transit operator, but such behaviour seems to be increasingly tacitly accepted as part of a doctor’s craft
By Garance Fannie Upham Chief Editor AMR-Times Geneva, Switzerland
Antimicrobial resistance (AMR) poses a serious threat to public health, growth and global economic stability. We affirm the need to explore in an inclusive manner to fight antimicrobial resistance by developing evidence-based ways to prevent and mitigate resistance, and unlock research and development into new and existing antimicrobials from a G20 value-added perspective, and call on the WHO, FAO, OIE and OECD to collectively report back in 2017 on options to address this including the economic aspects. In this context, we will promote prudent use of antibiotics and take into consideration huge challenges of affordability and access of antimicrobials and their impact on public health
G20 Leaders Communique, Hangzhou Summit 4-5 September 2016, point 46
By Fifa Rahman Postgraduate Researcher, University of Leeds, UK
Uptake of biosimilars, i.e. cost saving highly similar versions of the stiff price reference biologic products, has been slow throughout most of Europe and the rest of the world. Without express and official government policy purchasing and recommending biosimilars, doctors will not use biosimilars and the resulting cost savings cannot be made
By Yves Charpak MD, Public Health Specialist, PhD in Epidemiology
Blood transfusions are today safer than any other treatment procedures today in the richest part of the world. But it is less true elsewhere, where the role of unsafe blood transfusions on major dramatic epidemic situations is certainly high although not so well documented: hepatitis B and C and E... and even HIV...it is estimated by WHO (The World Health Organization) that up to 80% of the world population who need safe blood products don’t get them
By Marieke Bak Research Intern at AFEW International
A large international study among gay men and transgender women,the so-called iPrEx trial, suggested that pre-exposure prophylaxys (PrEP) by a tenofovir/emtricitabine combination can reduce the risk of HIV infection by at least 92% when the pills are taken consistently. Other trials subsequently confirmed PrEP effectiveness. PrEP is not intended as a stand-alone intervention, but rather as part of a multi-faceted strategy involving the use of condoms as well as regular follow-ups including for HIV and other sexually transmitted diseases testing
By Alphonse Kitoga Secretary General, Grands-Lacs en Action pour la Paix et le Développement Durable -The Great-Lakes in Action for Peace and the sustainable Development GLAPD_ Africa, asbl
La République démocratique du Congo continue à être confrontée à une crise humanitaire de très grande ampleur, et cela depuis plus de deux décennies, bien que la grande majorité du territoire nationale demeure stable, mais les provinces du Sud-Kivu, du Nord-Kivu, du Tanganyika et du Kasaï central sont les théâtres des tueries, massacres et violations répétitives des droits de l’homme à l’heure actuelle
By Muhwezi Edward Harm Reduction Counselor, Uganda Harm Reduction Network
The essence of the Uganda's Narcotic Drugs and Psychotropic Substances (Control) Act (NDPSA) is to treat people who use and inject drugs (PWUIDs) as criminals who need to be locked up instead of viewing them as human being in need of assistance. The criminalisation of drug use has had the effect of limiting the range of medical intervention available and accessible to PWUIDs in both private and public facilities. There is no comprehensive facility for the provision of public health services to PWUIDs. There is also no treatment available within Uganda for people who are on drugs and need critical and urgent medical attention like opioid substitution therapy. And there is a direct link between the criminalisation of drug use and HIV/AIDS as well as mental health challenges
By Anne-Emanuelle Birn Professor of Critical Development Studies, University of Toronto, Canada. and Judith Richter Affiliated Senior Researcher, Institute of Biomedical Ethics and History of Medicine, University of Zurich, Switzerland
Collective activism to overturn philanthrocapitalism’s hold on global health is an urgent necessity. This effort should draw from, and build upon, the resistance to the UN’s promotion of “multi-stakeholder partnerships” and neoliberal global restructuring since the 1990s. Those actors who have contributed either unwittingly, or through silent assent, or even with active collaboration, to the global health plutocracy also share responsibility in re-democratizing it
By Rebecca Barlow-Noone Student, University of Leeds, UK
To establish sustainable access to insulin in Cameroon, it is an imperative that reliance on pharmaceutical aid is revoked in favour of prioritising compulsory licensing and biosimilar usage. Until Novo Nordisk’s monopoly is challenged, patients will remain in uncertainty over access to insulin and essential equipment
By Bukenya Denis Joseph Human Rights Research Documentation Centre (HURIC) Kampala, Uganda
The issue to ponder about is who is this TRIPS meant to protect? Is it protecting the LDCs or the Developed Countries? The views I am trapping out there imply that the Agreement intends to protect creativity and the manufacturers so that they can expand their potential and motivate them in research. The least developed countries, Uganda inclusive need time to overcome the constraints preventing them from creating viable technological bases and Intellectual Property (IP) Laws. The IP Laws in Uganda are so muddled that they curtail the availability of affordable generic drugs in the country. Uganda as a nation would use a good training to the officers of the law in the IP section and also there is a need for increased materials on IP to be circulated amongst the health rights activists and advocates
By Matteo Zignol and Mario Raviglione Global Tuberculosis Programme, World Health Organization
Testing of resistance to isoniazid, pyrazinamide and fluoroquinolones is of paramount importance to guide treatment decisions and ensure that patients receive the best standard of care and have the highest chances to be cured. In this report the authors present an overview of the prevalence of resistance to isoniazid, pyrazinamide and fluoroquinolones and discuss the need of rapid diagnostics to detect resistance to these drugs
By Katherine Eve Young MD, MSc, MPH Manager Pricing & Market Access Creativ-Ceutical and Mondher Toumi Professor of Public Health University of Aix-Marseille, and CEO at Creativ-Ceutical
The current EU policy has a low ability to align access to orphan drugs across different Member States, leaving high inequity, especially between richer and poorer countries...The variation stems from the fact that although the marketing authorisation of drugs is at the European level, pricing and reimbursement decisions, and therefore patient access, are on a national level...Perhaps, to assure equal access to orphan drugs for all rare diseases, an EU-wide procurement should be considered...The EU can procure orphan drugs centrally and charge the MS based on their affordability while setting a fixed pan-European list price. Ultimately this will result in a differential pricing scheme
By Richard Howe Application Dynamics School of hard knocks, aviation trades, pilot and aircraft mechanic Punta Gorda, Florida USA
Richard Howe writes: Only one aircraft equipped with a pair of high pressure aerosol generators would be capable of treating over one million acres per night, using only 1/10 of the recommended amount of insecticide
By Ted Schrecker Professor of Global Health Policy, Newcastle University, UK Co-editor, Journal of Public Health
The idea of the 'Anthropocene' as an epoch with unprecedented scale, scope and interactions of multiple human impacts on the biosphere, can serve as a 'window' into crucial issues related to the connections among climate change, environment and health. In such contexts, integration of the fields of environmental ethics, public health ethics and bio(medical) ethics is needed
By Clara Affun-Adegbulu Intern and Research Assistant at Institute of Tropical Medicine in Antwerp (ITM)
Nicaragua currently lags behind other countries in the LAC region as for the decline of teenage pregnancies, and although the adolescent fertility rate fell sharply between 1990 and 2000, the decline has slowed considerably
By Jitendra Panda Country Director at Health Poverty Action Universitat Oberta de Catalunya, Somalia
Over 200 million girls and women living across 30 countries mainly in Africa as well as Middle-East and Asia share a common misery called genital mutilation / excision also known as female circumcision or Female Genital Mutilation (FGM). An additional 30 million girls are on the verge of submitting themselves into this practice in the coming decade.....The true extent of the abuse against children beginning as young as 7 and 9 years is much more than what we see in the numbers
By Kishore Shintre Food Fortification Consultant, ‘Hamara Prayatan’ (‘Our Efforts’) NGO, New Delhi, India
Tackling Severe Acute Malnutrition (SAM) among children has been a big challenge faced by several developing nations including India for decades now. Many Indian states have tried to use the packaged Ready to Use Therapeutic Food (RUTF) supplied by a few manufacturers (Indian and overseas) with limited success. Owing to the strong resistance put up by the Government Departments as well as the ‘Anganwadi ‘(Children Community) workers together with other associated people in implementing this effort due to variety of reasons it becomes imperative that we think of alternatives. One of them is producing freshly made RUTF at community level using the locally available food ingredients thereby making the food more palatable, easy to administer without changing the food habits of the children. This article deals with our experiment of creating this RUTF locally at community level tried out by our NGO Hamara Prayatan through research and development carried out at our laboratory
By Zoltán Massay-Kosubek Policy Manager for Health Policy Coherence at the European Public Health Alliance (EPHA)
High medicine prices is a key public health challenge in Europe and Trade policy – an exclusive EU competence can improve or exacerbate the situation. Free Trade and Investment agreements can make easier or harder for European governments to change existing policies to curb the costs of pharmaceuticals. Following a civil society dialogue meeting with EU Trade Commissioner Cecilia Malmström, the author is calling for policy between public health and trade goals on medicines, giving a priority to population health
By Angela Owiti Trainee at Wemos foundation
Global Health Initiatives such as GAVI, GFATM and PEPFAR have incurred criticism of being selective and narrowly defined while placing poor emphasis on - and falling short of - health systems strengthening
By Taye T. Balcha, MD, PhD, MPH Director of Armauer Hansen Research Institute in Addis Ababa, Ethiopia, and Donna A. Patterson, PhD Director of Africana Studies and Associate Professor of History at Delaware State University, USA
The authors turn the spotlight on the root causes of the rise of antibiotic resistance worldwide at a time when a global shortage of antibiotics has been reported by the WHO. Relevantly, the article emphasizes some solutions and calls on philanthropies, non-government organizations, regional institutions, states, and the private sector to work together and defeat the global threat posed by superbugs
By Muhammad Usman Khan WFP’s Technical Consultant to Planning and Development Department
...Still, the fact that doctors hold power over their patients is indisputable. One of the fundamental duty/responsibility of governments, medical boards and hospital administrations in this regard is/should be to ensure that rules are put into place in order to diminish the probability of any abuse of this power...
...there are serious institutional questions that need to be addressed here and patient-doctor interaction is more complicated than we would like to believe...
...We need to develop a policy framework within which the various facets of patient-doctor relationship are analysed and which forms the basis for nationwide guidelines that help doctors to understand their roles and responsibility better in their social media interactions...
By Karen Mancera-Cuevas MS, MPH, CHES Senior Project Manager at Northwestern University, Feinberg School of Medicine, Chicago USA
Resolving disparities in access to health care suffered from Latinx who reside in the U.S. includes the ability to understand the barriers created as a consequence of limited acculturation which is further compounded by social determinant of health indicators such as living situation, education, and access to social capital
By Philip J. Gover Director of Health Squared, Phnom Penh and G.J. Daan Aalders Media Intelligence advisor / entrepreneur, Amsterdam
How we think about and view health problems, and what we do about them as a result, is largely determined by how they are reported by television, radio, newspapers and social media. This article refers to a recent study whereby reports by two Cambodian newspapers across a range of key public health issues were analysed in terms of inclusion or absence of Positive Preventative Messages-PPMs (meaning any additional information enabling the reader to understand how the outcome of a story may have differed). As the authors maintain, PPMs shouldn’t be given up since using only naked facts denies the reader of critical information that could help improve health and health literacy
The contributions highlighted above add to PEAH internal articles published throughout the year in English or Italian language. Find the links below to English language collection:
Taking a Pill: Not So Counted On in South Africa
Do the Credit Policies of the WB, IMF & EC Damage Health?
Review: Textbook of Global Health
The Venezuelan Powder Keg Floods in the Neighboring Countries
Brazil Crippled by Corruption
EU to Get Rid of Big Pharma-friendly SPCs
Repealing Non-Violation Provisions under TRIPS
See also the following links to Italian language articles:
Oltre il PIL per la Misura del Benessere Globale
Proteggere i Diritti Terrieri delle Comunità Indigene per Salvare il Pianeta
Diritto alla Salute: il Ruolo Vitale della Legge
Antibiotico-resistenza: la risposta OMS
‘Orphan Drugs’ Business negli USA: un Monopolio Legalizzato
70ma Assemblea Mondiale OMS Risoluzioni Principali
Sesta Conferenza OMS Ambiente e Salute
Operativi in Italia gli Indicatori BES
In the meantime, our weekly page Health Breaking News Links has been serving as a one year-long point of reference for PEAH contents, while turning the spotlight on the latest challenges by trade and governments rules to the equitable access to health in resource-limited settings.
——————————————————
*Daniele Dionisio is a member of the European Parliament Working Group on Innovation, Access to Medicines and Poverty-Related Diseases. He is an advisor for “Medicines for the Developing Countries” for the Italian Society for Infectious and Tropical Diseases (SIMIT), and former director of the Infectious Disease Division at the Pistoia City Hospital (Italy). Dionisio is Head of the research project PEAH – Policies for Equitable Access to Health. He may be reached at d.dionisio@tiscali.it https://twitter.com/DanieleDionisio